





-

-
 23 jan 2021
23 jan 2021Thank you Rotary Club Beirut Cedars!

-
 25 nov 2020
25 nov 2020Bassma Communication on Engagement 2020
-
 02 sep 2020
02 sep 2020When President Macron meets few NGOs in Lebanon!
-
 17 sep 2018
17 sep 2018UNDP Latest Poverty Assessment Report: 30% of Lebanese are Poor
-
 09 feb 2018
09 feb 2018الكل في جريدة لنصنع وطنا
-
 09 nov 2017
09 nov 2017The world's food import bill is rising despite large production
-
 01 nov 2017
01 nov 2017If all societies eventually crumble, could Lebanon be next?
-
 21 oct 2017
21 oct 2017Lebanon can't handle refugees anymore: economy minister
-
 12 jan 2017
12 jan 2017GivingLoop - New online platform donations by Zoomaal
-
 13 nov 2013
13 nov 2013Mills, bakeries agree to maintain price of flour
-
 13 nov 2013
13 nov 2013Health Ministry sponsors week of free diabetes testing
-
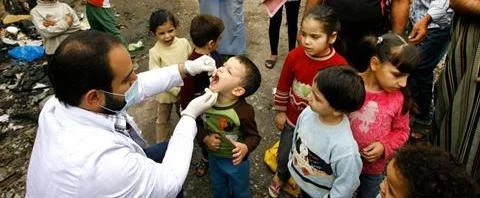 08 nov 2013
08 nov 2013Polio vaccination campaign kicks off in Sidon
-
 06 nov 2013
06 nov 2013Lebanon girl celebrates birthday with canned food drive
-
 01 nov 2013
01 nov 2013Renovations finally begin on nation’s ‘dangerous’ public schools
-
 29 oct 2013
29 oct 2013Syrian Refugees Now Equal One-Third of Lebanon’s Population
-
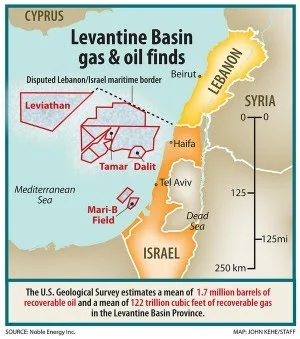 27 oct 2013
27 oct 2013Lebanon says gas, oil reserves may be higher than thought
-
 23 oct 2013
23 oct 2013The exodus of Lebanon’s nurses
-
 23 oct 2013
23 oct 2013Lebanon gasoline prices slightly up
-
 22 oct 2013
22 oct 2013Weighing the scales of justice for drug crimes
-
 22 oct 2013
22 oct 2013Hale says U.S. aims to increase Lebanon aid
-
 10 oct 2013
10 oct 2013Kuwait''s contributions to Lebanese health sector "unique" - official
-
 10 oct 2013
10 oct 2013بهذا المدخول.. تعيش عائلات لبنان
-
 09 oct 2013
09 oct 2013Lebanon gasoline prices continue to drop
-
 09 oct 2013
09 oct 2013Lebanon’s first outdoor public gym opens in Jbeil’s Wagon Park
-
 07 oct 2013
07 oct 2013After shipwreck, Lebanese survivors return to poverty
-
 03 oct 2013
03 oct 2013Lebanon students wasting less food
-
 21 sep 2013
21 sep 2013Syria war, refugees to cost Lebanon $7.5 billion - World Bank – 19-Sept-2013
-
 18 sep 2013
18 sep 2013Lebanon gasoline prices drop after weeks of increases
-
 11 sep 2013
11 sep 2013Lebanon gasoline prices rise once more
-
 02 sep 2013
02 sep 2013HSBC cuts back in Lebanon, Jordan, Bahrain
-
 02 sep 2013
02 sep 2013Demand for anti-anxiety meds still high
-
 27 jul 2013
27 jul 2013Courts Suppressing Smoking Ban
-
 02 aug 2013
02 aug 2013Study: Hotter temperatures lead to hotter tempers
-
 02 aug 2013
02 aug 2013Mers: New virus 'not following Sars' path
-
 31 jul 2013
31 jul 2013World Bank Project to Improve Lebanon’s Mobile Internet Services
-
 02 aug 2013
02 aug 2013Lebanon's forgotten child laborers
-
 24 jul 2013
24 jul 2013Crocodiles Spotted in Beirut River
-
 25 jul 2013
25 jul 2013Lebanon's Teacher Layoffs
-
 25 jul 2013
25 jul 2013Microfinancing among the poor
-
 08 jul 2013
08 jul 2013Addressing social, economic inequalities crucial to achieve sustainability – UN officials
-
 25 jul 2013
25 jul 2013Lebanon Affected by Refugee Crises
-
 25 jul 2013
25 jul 2013Timing of first solid food tied to child diabetes risk
-
 17 jul 2013
17 jul 2013UCC launches petition drive for wage hike
-
 25 jul 2013
25 jul 2013Joblessness in the Middle East
-
 10 jul 2013
10 jul 2013Does a Child Die Every 10 seconds?
-
 10 jul 2013
10 jul 201338 countries meet anti-hunger targets for 2015
-
 10 jul 2013
10 jul 2013Ginger Destroys Cancer More Effectively than Death-Linked Cancer Drugs
-
 29 jun 2013
29 jun 2013As Doctors Leave Syria, Public Health Crisis Looms
-
 03 jul 2013
03 jul 2013Both Residents and Refugees are Struggling in Lebanon
-
 06 jun 2013
06 jun 2013Lebanon: Banks central to counter Syrian crisis
-
 26 jun 2013
26 jun 2013Lebanese mothers bothered by promotion of formula milk
-
 02 jul 2013
02 jul 2013What Lebanon must do to reach its 2015 Millenium Development Goals
-
 02 jul 2013
02 jul 2013Beirut: Public Transport Rivals Paralyze Reform
-
 02 jul 2013
02 jul 2013Cyprus Crisis Sparks Lebanese Bank Anxiety
-
 02 jul 2013
02 jul 2013Beirut Stock Activity Down
-
 29 may 2013
29 may 2013Fouad Boutros highway project highly debated
-
 02 jul 2013
02 jul 2013WHO: One third of all women face violence
-
 28 jun 2013
28 jun 2013Committee to treat drug addiction offers new hope
-
 27 jun 2013
27 jun 2013Pledge to improve nutrition signed
-
 25 jun 2013
25 jun 2013Lebanon moves to shut down illegal eateries
-
 25 jun 2013
25 jun 2013Real estate transactions down more than 8 pct
-
 06 jun 2012
06 jun 2012Where does your meat come from?
-
 25 jun 2013
25 jun 201316 Hours of electricity promised this summer
-
 14 jun 2013
14 jun 2013Like traffic, Jal al-Dib tunnel plans at standstill
-
 21 jun 2013
21 jun 2013Gasoline prices continue to rise
-
 21 jun 2013
21 jun 2013Public debt reaches $59 billion in April
-
 21 jun 2013
21 jun 2013First lady inaugurates women's cardiovascular center
-
 21 jun 2013
21 jun 2013Beirut retail sales plunge 14.4 percent in first quarter of 2013
-
 21 jun 2013
21 jun 2013Sleiman signs wage hike
-
 07 jun 2013
07 jun 2013Achrafieh Residents Save Their Park
-
 11 jun 2013
11 jun 2013U.N. launches campaign to combat food waste
-
 03 jun 2013
03 jun 2013Most Beirut properties completed in 2012 unsold
-
 04 jun 2013
04 jun 2013Stock market activity down 30% to $89m in first four months of 2013
-
 10 jun 2013
10 jun 2013Lebanon’s beaches are toxic
-
 05 jun 2013
05 jun 2013Gas Prices Go Up at Start of June
-
 29 may 2013
29 may 2013Gasoline prices continue slight rise
-
 28 sep 2012
28 sep 2012Nearly 30% of gastroenteritis-related hospitalizations among children under five in Lebanon are due to Rotavirus
-
 20 may 2013
20 may 2013Power rationing jumps to 9 hours in Beirut
-
 21 may 2013
21 may 2013Bank Audi warns over Lebanon’s rapidly increasing public debt
-
 22 may 2013
22 may 2013Demand for cheaper cars reflects weaker purchasing power
-
 22 may 2013
22 may 2013Lebanon gasoline prices up slightly
-
 20 dec 2012
20 dec 2012Are Lebanese children too short?
-
 27 sep 2012
27 sep 2012Annual use of mammogram to detect breast cancer is on the rise in Lebanon
-
 24 mar 2013
24 mar 2013Approval of public-sector wage increase puts at risk the sustainability of public finances
-
 11 apr 2013
11 apr 2013Consumer Confidence in Lebanon drops to Near Record Low in Second Half of 2012
-
 23 may 2013
23 may 2013World Bank approves $30m for social protection project
-
 21 may 2013
21 may 2013Keeping Kids in School with Meals Program
-
 21 may 2013
21 may 2013Gas Prices Remain the Same
-
 21 may 2013
21 may 20134G arrives to Lebanon!
-
 24 apr 2013
24 apr 2013Lebanon gasoline prices see significant drop
-
 26 apr 2013
26 apr 2013Medical organizations announce vaccine campaign
-
 19 apr 2013
19 apr 2013Alfa, touch to reduce rates for 3G services
-
 23 apr 2013
23 apr 2013Lebanese gas to enter crowded market
-
 25 apr 2013
25 apr 201360 Students Hospitalized over Water Contamination in Tripoli
-
 11 apr 2013
11 apr 2013The sinister side of Lebanon’s electricity crisis
-
 09 apr 2013
09 apr 2013Many Lebanese elderly socially isolated
-
 04 feb 2009
04 feb 2009Thank you SOS Chrétiens d'Orient!
-
 07 jan 2025
07 jan 2025Thank you SOS Chrétiens d'Orient!